

Background: Early death (ED) during first-line therapy for acute myeloid leukemia (AML) is acknowledged as a pending issue worldwide. Few pivotal studies from developed countries have identified baseline characteristics related to poor outcome. Retrospective reports from Brazil and Mexico indicate alarming ED rates from real-world data, raising the question of which factors contribute towards this finding in low-income centers. In this study, we aimed to identify risk factors for ED in AML to increase the prediction power of previously known tools such as Charlson's Comorbidity Index (CCI) as well as to examine the role of anti-infective prophylaxis in our cohort.
Methods: This is a retrospective cohort study involving adult patients (pts) newly diagnosed with AML treated at Instituto do Cancer do Estado de Sao Paulo, Brazil between June 2011 and June 2020. Only pts receiving the classic "7+3" regimen were included. We used a slight modification of European LeukemiaNet 2010 classification previously published by our group - Adapted Genetic Risk (AGR) (Silveira et al., 2020). The primary endpoint was ED rate, calculated by the Kaplan-Meier method. A Cox regression model selected by a stepwise method was used to find risk factors. Post-chemotherapy events (secondary endpoints) constituted any documented infection, bleeding, thrombosis, and acute kidney injury (AKI) during the first 30 days.
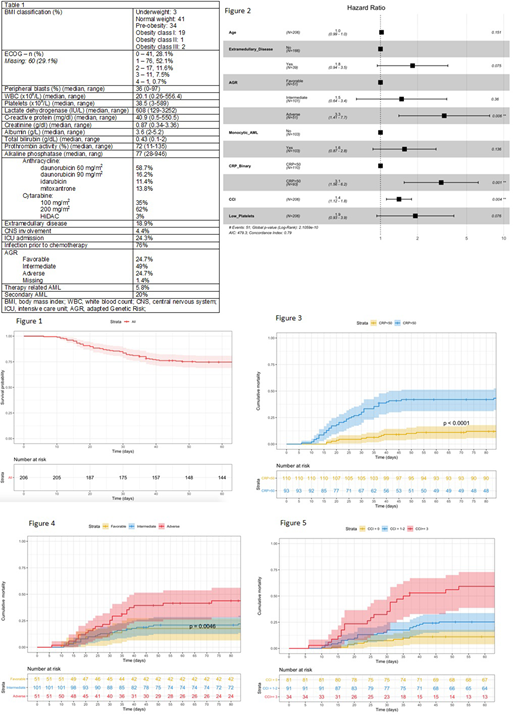
Results: Overall, 206 out of 337 pts (61%) entered in the analysis. The median age was 54 years (range,17-74) and 50.5% were male. The median time between symptoms' onset and hospital admission was 7 weeks (0-48). Thirteen pts (6.3%) presented with leukostasis, of which 9 proceeded leukapheresis. At the presentation, clinical tumor lysis syndrome was seen in 12% of patients (associated with extramedullary disease [p<0.001], among other factors). Other baselines clinical and laboratory findings are summarized in table 1. Pre-chemotherapy infection was found in 67% of patients (positive blood culture: 26.3%). 45-day mortality was 23.8% (95% CI 17.8-29.4) (Figure 1), being 39.8% in pts above 60y. Dose reductions for liver or kidney dysfunction were not, per si, associated with higher ED. Multivariable Cox regression models examined the utility of baseline markers in predicting ED in our cohort and the best-fitted model by Akaike information criteria (AIC) is outlined in a forestplot (Figure 2). Briefly, in a model controlled for age, adding phenotype, genetic risk, platelets and C-reactive protein (CRP) to CCI resulted in improved prediction in our cohort (AIC 479 vs 542). CRP, AGR, and CCI were independently associated with short-term survival in AML (figure 3, 4, and 5). Noticeably, 13/20 diabetic patients died during the first 45 days (unadjusted HR 4.29 [95% CI 2.33-7.92]). Only antibacterial prophylaxis with quinolone was associated with decreased ED (unadjusted HR 0.38 [95% CI 0.15-0.95]), while the use of fluconazole or anidulafungin did not affect survival. Colonization during hospitalization occurred in 71% (mainly vancomycin-resistant Enterococcus [77%] and carbapenemase-producing Enterobacteriaceae [44%]). Any sort of colonization was associated with ED (OR 4.41 [95% CI 1.89-12.08]). Thromboembolic events were registered in 11.9% (95% CI 7.9-17.4, mostly catheter-related) and were marginally associated with central nervous system disease (OR 4.31 [95% CI 0.84-18.25) and diabetes mellitus (DM) (OR 3.24 [95% CI 0.94-9.82) 20.8 vs 7.9%, p=0.097). Bleeding was observed in 17.6% and was associated with monocytic AML subtypes, tumor lysis, and DM. Complete response was attained in 50.5% (95% CI 43.4- 57.5). Presumed or confirmed invasive fungal infection was diagnosed during induction in 26.6%, but empirical amphotericin was prescribed in 60.2%. 66.5% of subjects developed any grade of AKI, with the need for hemodialysis in 10.3%.
Conclusion: This is the first Brazilian study to evaluate risk factors for ED in newly diagnosed AML in the public setting, as well as to address which events explain such higher mortality in comparison to American and European reports. In line with the literature, age itself was not associated with mortality when adjusted for other variables such as CCI and genetic stratification. Interestingly, we found that the baseline CRP levels are significantly correlated with ED, highlighting the role of infection and inflammation at the AML diagnosis.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal